Understanding Knee Replacement
Arthritic knee pain is a painful condition that can severely restrict activity and quality of life. Typical symptoms of knee arthritis include aching, stiffness, and difficulty walking. Patients suffering from this condition are unable to participate in desired activities due to knee pain and dysfunction. The knee is often painful with any prolonged walking and can feel weak or unstable during everyday life. The most common cause of knee pain in patients over 40 is osteoarthritis which is a degenerative condition of the knee involving loss of cartilage with resultant inflammation, pain, and loss of function. Other causes of knee pain include post-traumatic arthritis, rheumatoid arthritis, and avascular necrosis. All of these conditions lead to a common final outcome of chronic pain within the knee associated with pain, stiffness, swelling, and inability to perform activities of daily living.
Going back several decades there was no definitive treatment for patients suffering with chronic pain due to knee arthritis. Patients either gave up normal activity or were severely limited due to pain. Fortunately, modern medicine for years worked to create a solution to this condition and finally in 1968 the first modern knee replacement surgery was performed. Since that time the technology and technique of knee replacement surgery have evolved significantly. There have been major improvements in the actual prosthetic design of the knee implant to reduce mechanical wear, improved function, and increase the longevity of the prosthesis. The surgical technique has evolved such that many patients who formerly would have been hospitalized for several weeks after total knee replacement now go home within a few hours after surgery from an ambulatory surgery center (ASC). Surgeons remain committed to continuing this process of improvement in order to better serve patients in the years to come.
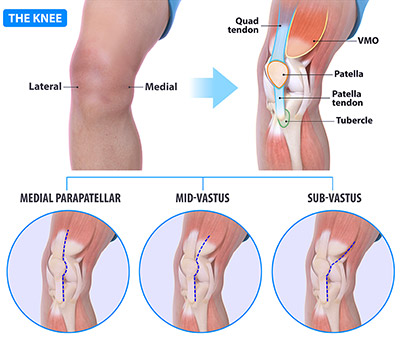
So what exactly is meant by the term “total knee replacement”? Many outside observers assume that this surgery entails the removal of the entire knee joint along with surrounding ligament, tendons, and bone. However, the truth is that surgeons seek to preserve as much of the native bone and tissue as possible. During a knee replacement the surgeon will expose the knee through one of several basic approaches. The Medial parapatellar arthrotomy is the most traditional often a midline incision over the front of the knee as well as cutting the quadriceps tendon in order to enter the knee. The midvastus approach to knee replacement involves exposing the knee by splitting (cutting) the muscle of the vastus medialis in line with its fibers. Both of these approaches can result in slightly increased postoperative pain due to cutting through either major tendon structures around the knee or the surrounding musculature. The more recently popular SubV Knee (subvastus approach) is a minimally invasive approach that involves exposing the entire knee while simultaneously avoiding cutting any of the adjacent muscle or tendon. The approach for the SubV Knee involves an incision slightly medial (to the inside) of the midline of the knee with the proximal incision curving medially over the muscle belly of the vastus medialis musculature. The SubV Knee is typically performed by surgeons who are experts in knee replacement surgery due to the experience level necessary to perform the SubV Knee without complication. Most surgeons consider the SubV Knee (subvastus approach) to be the most minimally invasive approach to knee replacement surgery yielding overall less pain and a quicker recovery.
After exposure of the knee through the SubV approach the surgeon will then carefully remove small amounts of bone, typically 8-10 mm, from the end portion of both the femur and tibia in order to facilitate placement of the knee replacement prosthesis. The surrounding soft tissues are left intact including retention of nearly all ligaments and tendons around the knee. At this point the femoral and tibial implants are securely attached to the bone and a polyethylene (plastic) implant is locked into place in the joint to essentially recreate the smooth weight bearing surface that was formerly cartilage. In this way, the knee will now have metal articulating on plastic instead of bone rubbing against bone.

Most patients who are relatively healthy undergo SubV knee replacement surgery as an outpatient procedure with no need for hospitalization. These cases are performed at an Ambulatory Surgery Centers (ASC) with discharge often just a few hours after surgery. Before leaving the ASC patients must have pain controlled and have met physical therapy goals which include being able to ambulate independently on a walker and climb stairs with minimal assistance. Patients typically start out on a walker for support after surgery however many are walking without any assistive device within 1-2 weeks. Return to work times vary based on the individual patient as well as workplace demands however many patients are back to office-based work within 5-7 days.
